September 5, 2024
Tesofensine A Review
Long-term Efficacy And Safety And Security Of Anti-obesity Treatment: Where Do We Stand? Current Weight Problems Reports A great number of these medications or mixes thereof have confirmed successful in dealing with alcohol and drug dependencies or other behavioral addictions such as trouble gambling. Homeostatic control centers in the hypothalamus and the brainstem are of particular value for metabolic Go to the website control. Both of these brain locations remain in close distance to circumventricular body organs (e.g., the typical renown or area postrema) that contain "leaking," fenestrated capillaries to enable gain access to of outer nutrients, metabolites, and hormones. The brainstem integrates temporary satiation signals from the GI system either straight using the blood, or using input from vagal afferents that innervate the esophagus, tummy, and small intestinal tract. The nerve ends respond to mechanical stimuli such as stomach dilatation, as well as to chemical satiation signals including the postprandially secreted GI hormonal agents cholecystokinin (CCK) (10 ), glucagon-like peptide-1 (GLP-1) (11, 12), peptide YY (PYY) (13 ), and apolipoprotein A-IV (ApoAIV) (14 ). After binding to certain receptors on the vagal afferents, all of these signals converge in the core of the solitary system in the brainstem and are consequently communicated to various other brain locations to be finally incorporated into result signals to induce satiety.Lasting Efficiency And Safety Of Anti-obesity Therapy: Where Do We Stand?
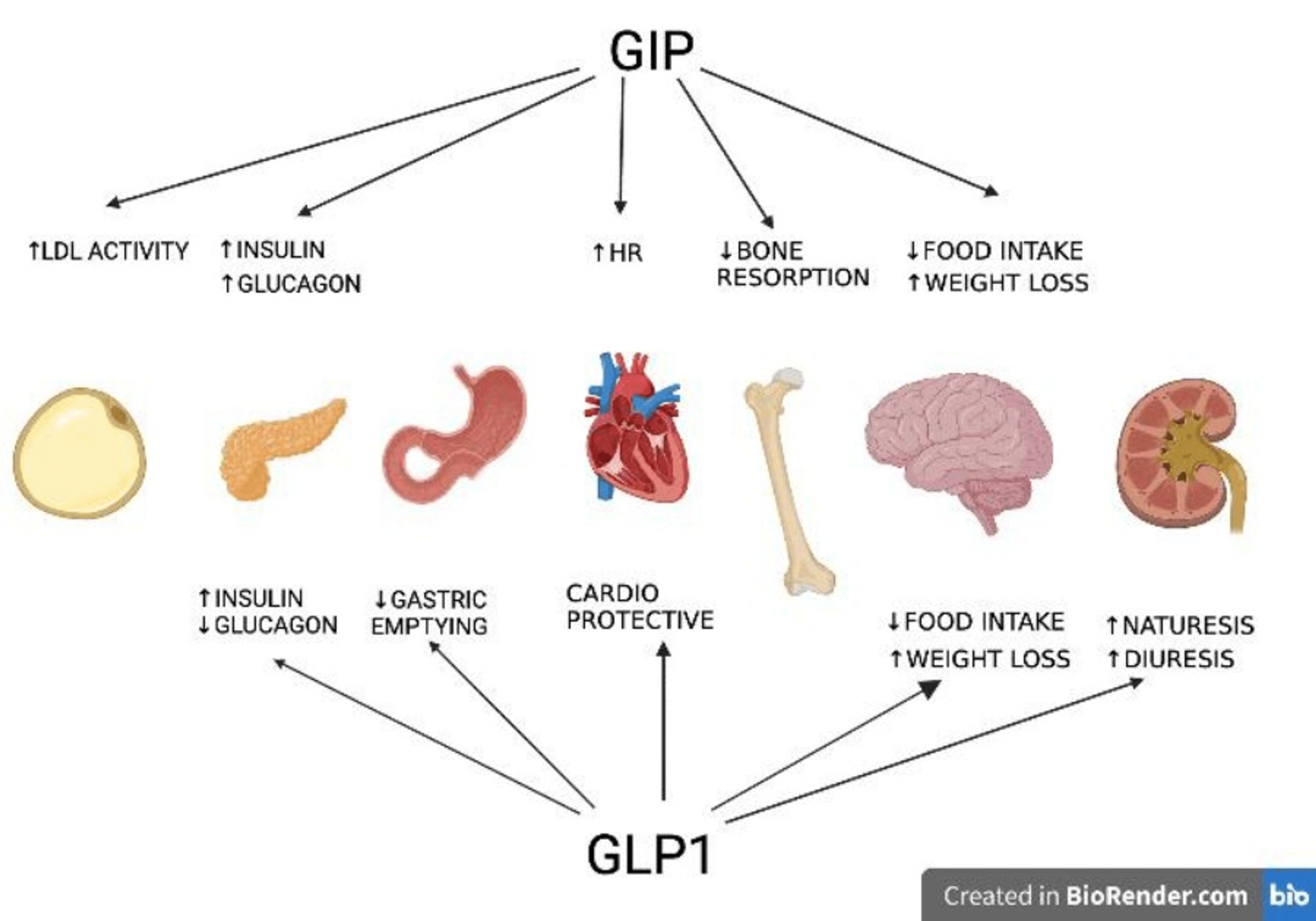
GIP blocks the emetic impacts of GLP1R agonism in musk shrews190 and near-normalization of blood glucose has been reported to recover the insulinotropic result of GIP in patients with T2D191. Moreover, GIP agonism improves adipocyte storage space capability to secure from adipocyte lipid spill over and ectopic lipid deposition192. Nonetheless, as gone over in the coming before subsection, making use of GIPR agonists for the treatment of weight problems and T2D is debatable. Up until lately, long-term pharmacotherapy to accomplish body weight normalization in addition to suitable tolerability and safety remained an overwhelming challenge34. However, recent medical trials with advanced healing candidates consisting of glucagon-like peptide 1 receptor (GLP1R) agonism are advertising the belief that advancement, drug-based monitoring of weight problems might be feasible.Tesofensine
- Sibutramine was approved by the FDA in 1997 however was taken out due to raising the danger of cardiovascular events in a risky population for which sibutramine's use was initially not intended154.
- In an 18-week test utilizing a tipped titration dosing procedure for MK-0493, the very same outcome was observed (Krishna et al., 2009).
- Extremely recently, it was shown that CNS loss of GIPR renders mice resistant to GIP-induced body weight loss, suggesting that GIP controls energy metabolism via CNS GIPR signalling185.
- The fine-tuning of melanocortin tone by competing neuropeptides inevitably controls ingestive behaviors and actions beyond feeding (76-- 78) as well as non-CNS procedures such as thermogenesis and WAT browning (79) or bone metabolic rate (80 ).
What is the most effective weight management therapy?
For individuals with a BMI over 35 & #x 2014; or a BMI above 30 with various other associated health problems & #x 2014; bariatric surgical procedure is frequently one of the most efficient lasting treatment for weight loss.
Peptide Tyrosine Tyrosine
A recent experience from the Sibutramine Cardiovascular End Results (SCOUT) trial clearly indicated that sibutramine administration ought to be purely avoided in clients with a background of heart disease, consisting of those with uncontrolled hypertension (14,15). One more prominent failing of an AOM was sibutramine-- a norepinephrine and serotonin reuptake inhibitor that lowers cravings and promotes thermogenesis. Sibutramine was approved by the FDA in 1997 however was taken out as a result of boosting the risk of cardio occasions in a high-risk populace for which sibutramine's usage was originally not intended154. This increase in blood pressure and pulse rate wasreversed by a beta-1-adrenergic obstructing medication without affecting thereduction in food consumption. An angiotensin blocker did not impact the decrease infood intake, however only partially blocked the rise in blood pressure and pulserate suggesting that tesofensine might boost thoughtful task [124] A stage III test will be completedin 2018 to study adjustment in body weight in 372 grownups with excessive weight treated withplacebo, 0.25 mg or 0.5 mg tesofensine for 24 weeks. Agonists of NPY Y2 and Y4 receptor subtypes have also been evaluated after it was found that the digestive tract hormonal agent, peptide YY (PYY), decreased food consumption by stimulating hypothalamic Y2 receptors. Numerous groups have actually reported that infusion of PYY3-- 36 lowered food intake in lean and overweight topics when provided acutely (Kamiji and Inui, 2007). Nevertheless, because this molecule is a polypeptide, finding an application formula suitable for repeated administration presented a substantial issue. 

Social Links