Fat Burning: Leading 3 Ways To Deal With Weight Problems
Anti-obesity Drug Discovery: Breakthroughs And Difficulties Nature Assesses Medicine Exploration Extremely recently, it was shown that CNS loss of GIPR provides computer mice resistant to GIP-induced body weight reduction, showing that GIP manages basal metabolism through CNS GIPR signalling185. Substantiating the significance of this finding, it is noteworthy that the exceptional weight-lowering effect of MAR709 relative to a GLP1 monotherapy of matched structure and pharmacokinetics disappeared in CNS Gipr knockout mice185. The main devices and target regions for GIP harmony with GLP1 remain to be determined, and notably there are clashing preclinical results that advertise GIPR animosity as a therapeutic choice for treating obesity184. Amylin (also known as IAPP) is a peptide that is co-secreted with insulin and decreases food intake through central control of satiety pathways231,232 (Box 1; Fig. 2).
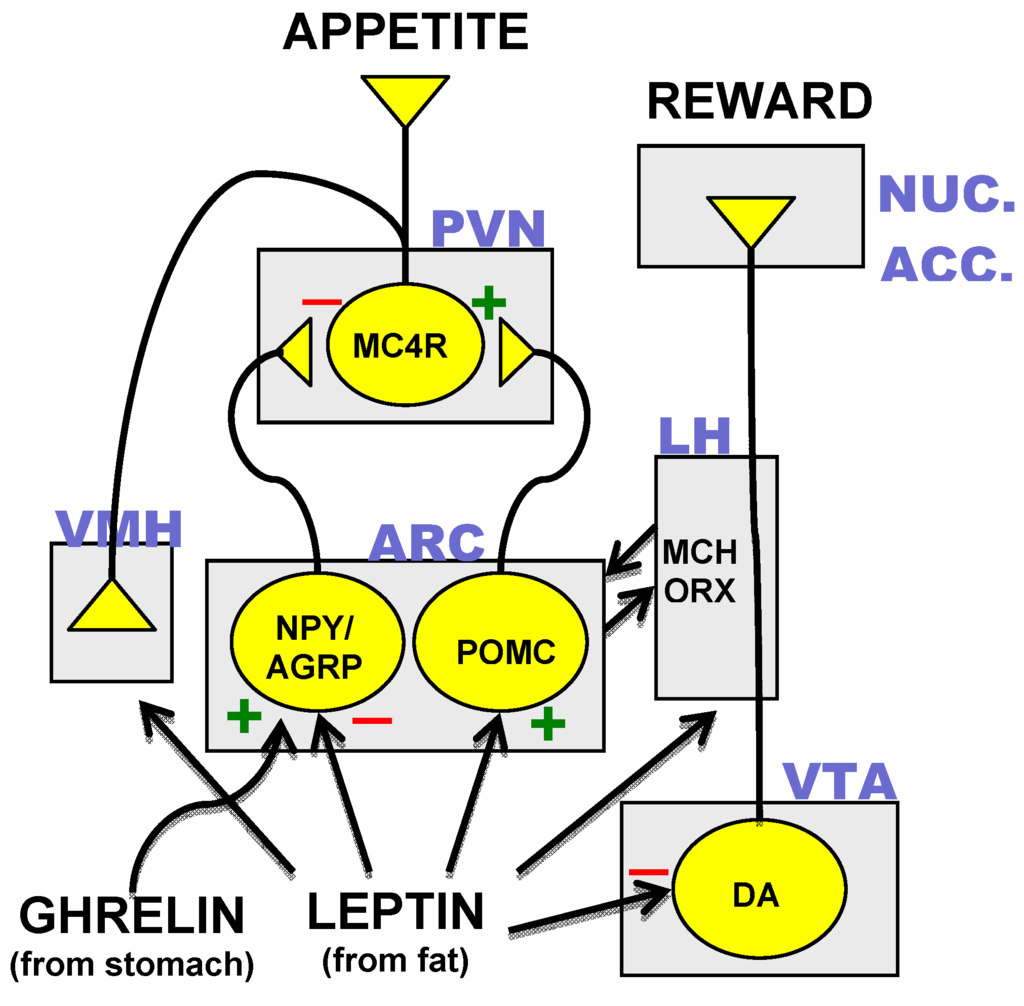
Main Regulation Of Food Consumption And Energy Expenditure
What is one of the most efficient weight loss therapy?
For people with a BMI over 35 & #x 2014; or a BMI above 30 with other associated health problems & #x 2014; bariatric surgical treatment is typically one of the most reliable lasting therapy for weight-loss.
Amongst suprasellar growths, craniopharyngioma is the most typical source of gotten hypothalamic weight problems, either directly or complying with medical or radiotherapeutic intervention. Today, treatment is restricted to methods to take care of excessive weight however with a moderate and variable impact. Present techniques consist of enhancing pituitary hormone substitute, calorie limitation, increased energy expenditure through physical activity, behavior interventions, pharmacotherapy and bariatric surgical treatment. Present pharmacotherapeutic approaches include stimulants that enhance energy usage, anti-diabetic agents, hypothalamic-- pituitary alternative therapy, octreotide, and methionine aminopeptidase 2 (MetAP2) preventions. Some pharmacological research studies of hypothalamic weight problems report weight management or stabilization however reported treatment periods are short, and others report no result. Unique or combined approaches to manage hypothalamic weight problems are hence called for to accomplish legitimate and sustained weight loss.
Do I Have To Be Incredibly Overweight To Take Advantage Of Medical Weight Loss?
Throughout a medically supervised weight reduction program, we have a team of professionals in Merritt Island who gauge a client's weight loss by the variety of pounds lost, their metabolic process, and body composition.
Certainly, imitating the effects of bariatric surgery has turned into one vision for discovery of future AOMs.
Much of the neuropeptide receptors revealed centrally are likewise shared peripherally and hence actions of agonists or villains of these receptors can not be presumed to generate weight reduction by central systems alone.
Naltrexone/bupropion (Contrave ®), a mix of medicines with 2 different systems, is used for the long-lasting administration of weight-loss.
She furthermore noted that long-term lifestyle changes and feasible long-lasting medication use might be essential to preserve weight-loss and decrease individuals's risk for obesity-related wellness problems. In conclusion, a number of brand-new techniques to the treatment of weight problems are presently in late stage growth and some appear, currently, to provide better efficacy and enhanced tolerability than existing treatment. Multiple users experienced habit forming habits that went beyond a simple habituation to the effects of amphetamines. Finally, there are recently reported successes in developing crossbreed medicines that utilize GLP-1 as a hormonally active peptide for the cell kind-- details shipment of chemically conjugated nuclear receptor agonists (146, 147) and antisense oligonucleotides (148 ). As an example, GLP-1R targeting has actually been leveraged to deliver estrogen to metabolically pertinent tissues, where it enhanced the body weight-- decreasing, insulinotropic, and islet-preserving effects of estrogen through corresponding pharmacology. Notably, endocrine poisonings in non-- GLP-1R-- revealing body organs were missing, which highlights the cell kind-- specific shipment (146, 149). A small research carried out in obese nondiabetic women with polycystic ovary syndrome showed that a mix of exenatide with metformin favorably affected body weight, insulin sensitivity, and menstruation cyclicity. These advantageous impacts were much more pronounced with mix therapy than with management either of exenatide or metformin alone (60 ). Advances in the medical development of CNS-acting weight problems medications haveresulted in currently available medicines that are capable of minimizing food intake, reducing desire, enhancing satiety and potentially increasing energy expense. Weare now in a phase of dealing with excessive weight with reduced dosage drug combinations actingthrough several monoamine paths. As evaluated in the section on presentlyavailable weight problems medications, two instances of these combination treatments mostrecently accepted are bupropion/naltrexone and phentermine/topiramate. As discussed formerly in section 2.3, a negative effects brought on by thenon-specific serotonin agonists, fenfluramine and dexfenfluramine, was heartvalve lesions, as a result of stimulation of the outer serotonin 2B receptor. In between 0.125 and lmg, there was a dose-dependent clog ofbinding, and striatal dopamine carrier occupancy ranged 18% and 77%. in a sigmoid- shaped Emax (optimum result attributable to the medicine) partnership. The sigmoid Emax version is a mathematical version that describes theconcentration- result partnership of a drug where the contour obtains more sigmoidin shape as the number of molecules binding to the medicine receptor increases. Themaximal tenancy was 80% and the dosage at half tenancy was 0.25 mg with a serumlevel of 4ng/mL. These results suggested that tesofenine-induced reduction infood consumption was partially mediated by up-regulation of dopaminergic pathways dueto blockade of presynaptic reuptake [120] Liraglutide 3mg is provided subcutaneously daily, and thedose is started at 0.6 mg and enhanced by that quantity weekly up until 3mg isreached. The medication is contraindicated while pregnant and in individuals with apersonal or household background of medullary thyroid cancer cells or several endocrineneoplasia type 2. There is sufficient evidence supporting that pharmacotherapy in combination with behavior-based treatments can result in considerable weight loss and enhanced cardiometabolism. Looking back with the history of obesity therapy, we note that thefirst reduced carb diet plan was the Banting Diet regimen, released in 1863. Diet plan still plays a vital role inweight loss, but longterm pharmacotherapies with limited negative effects are criticalfor maintaining fat burning. The very first jejunoileal bypass for obesity was reportedin the 1950's [128], and the operationdid not end up being prominent till the 1970's. Advanced treatments are usednow and surgical procedure still has a significant place in the treatment of obesity, givingthe biggest weight-loss, best upkeep of weight-loss, and turnaround of insulinresistance. This section on future anti-obesity medicines concentrates on tesofensine, because itis the only CNS acting anti-obesity medicine that has actually reached an advanced phase ofdevelopment.
Hello, and welcome to PharmaPioneer Solutions! I'm James Smith, the founder and lead pharmaceutical scientist here. My journey into the world of pharmaceuticals began at a young age, sparked by a childhood fascination with science and a desire to make a tangible impact on people's health.
After earning my Ph.D. in Pharmaceutical Sciences, I spent over a decade in various roles across the industry. From leading clinical trials that brought groundbreaking treatments to market, to navigating the complex pathways of FDA approvals, my career has been a blend of innovation, challenge, and reward.