September 5, 2024
Experts Comment On Study Into A Possible Brand-new Weight Problems Medicine, As Published In The Lancet
Tesofensine, An Unique Antiobesity Medicine, Silences Gabaergic Hypothalamic Nerve Cells Pmc Bariatric surgical treatment might produce continual weight-loss in some individuals (14, 15) yet is not an option for a lot of due to the fact that lasting security and malabsorption issues might present a difficulty (16, 17). In comparable tests of other anti-obesity medicines, net weight-loss of 2.9 kg, 4.2 kg and 4.7 kg have been accomplished with orlistat, sibutramine and rimonabant, specifically, over the exact same amount of time. So, the authors suggest that tesofensine 0.5 mg once daily for 6 months has the possible to cause fat burning two times that induced by presently approved medications, and Phase III trials are expected to start next year. At week 32, the AHI was significantly reduced, with weight management, in the liraglutide group than in the sugar pill (− 12.2 ± 1.8 occasions h − 1 vs. − 6.1 ± 2.0 occasions h − 1) [44] Amongst the clients that completed 4 years of therapy, the percentage of individuals who attained a minimum of 5% fat burning was dramatically higher in the orlistat group (52.8%) than in the placebo team (37.3%). At the end of the 4-year research, the collective incidence of diabetic issues was 9.0% in the placebo group and 6.2% in the orlistat team, with a threat decrease price of 37.3% [17]Pharmacological Support For The Treatment Of Excessive Weight-- Existing And Future
Is tesofensine an antidepressant?
- Lastly, one Tesomet-treated patient had re-growth of craniopharyngioma discovered by a pre-scheduled MRI-scan.
- Of these, qnexa seems the most effective, with the highest dosage achieving approximately 10 kg (9%) placebo-adjusted fat burning over 52 weeks with over 60% of participants shedding over 10% of their weight complying with an LOCF analysis.
- It has also shown effectiveness in therapy of gambling disorder along with alcohol and opioid dependency (Grant, Kim, & Hartman, 2008; Give, Odlaug, Potenza, Hollander, & Kim, 2010).
- The Mayo team performed a perennial clinical test performed in a weight management center where 312 people were randomly appointed to phenotype-guided therapy or treatment that was not phenotype guided and included anti-obesity drugs.
- Yet if consumers aren't specifically demanding the obesity drugs, there is plainly a demand for weight-loss products.
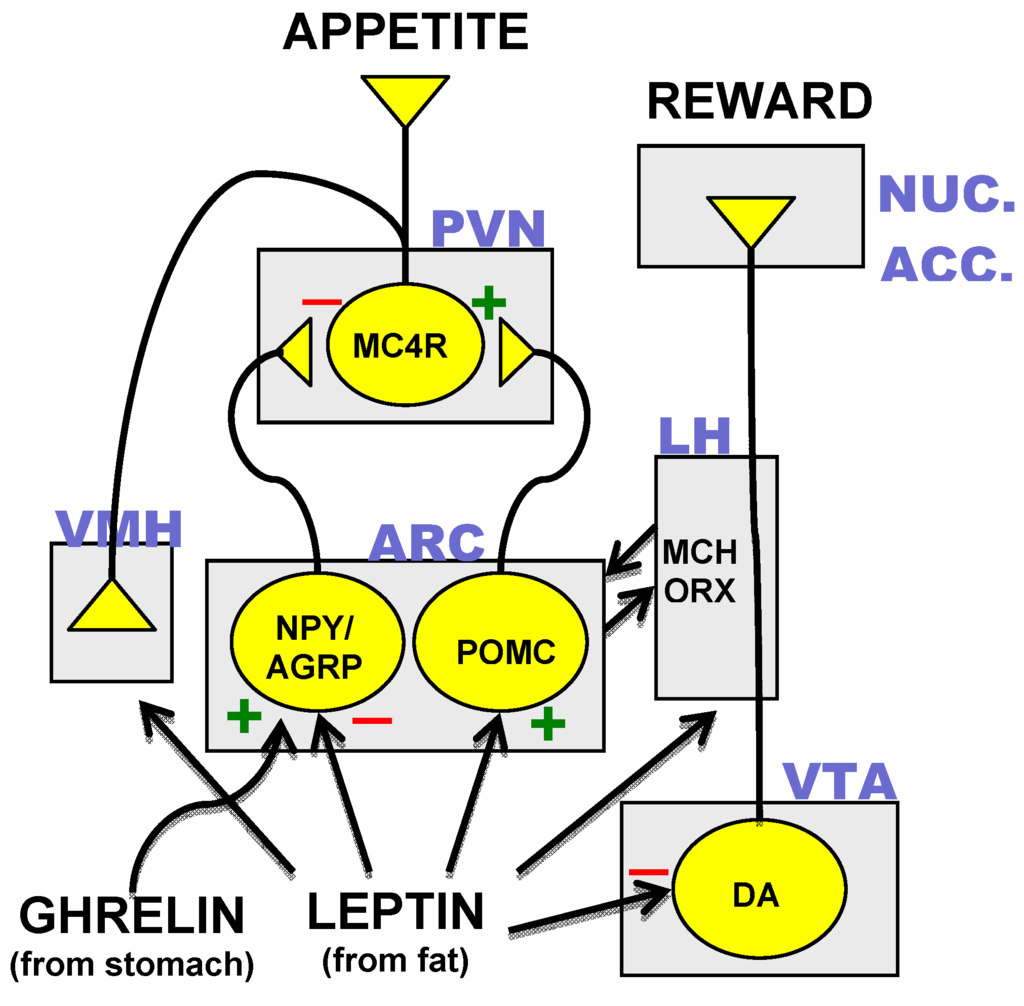
The Anorexigenic Results Of Tesofensine Are Amplified By The Chemogenetic Restraint Of Lh Gabaergic Neurons
In a small-scale clinical trial with 161 individuals, individuals who obtained either 0.5 or 1.0 mg of tesofensine for 24 weeks experienced weight decreases of 11.3 and 12.8 kg, respectively. The weight decrease was 2.2 kg in the sugar pill group, which indicates that tesofensine may have two times the weight reduction result of formerly developed medicines [74] The weight decrease impact of tesofensine can be credited to enhanced over night power expense and fat oxidization rate [75] Additionally, the use of tesofensine creates positive modifications in midsection circumference, insulin resistance, adiponectin, lipid profiles, and glycemic control. Nevertheless, the adverse effects of tesofensine consist of completely dry mouth, sleeping disorders, irregular bowel movements, nausea or vomiting, and a raised heart rate. Craniopharyngioma, one of the most typical cause of hypothalamic weight problems, has a general incidence of roughly 1.3-- 1.7 per million people/year (8, 9). Hypothalamic excessive weight creates in approximately 50% of craniopharyngioma survivors (10, 11). The major adverse effects of liraglutide are gastrointestinal signs and symptoms, such as queasiness, diarrhea, constipation, and throwing up, and it is recommended that the dosage is incrementally increased to reduce the occurrence of these adverse events. Owing to the delayed gastric draining triggered by liraglutide, the action of various other medications can be affected. Additionally, liraglutide use can create gallstones and, less generally, acute pancreatitis [57,58]; it should not be utilized in patients with a background of pancreatitis. Since there are problems concerning liraglutide use and medullary thyroid cancer cells and multiple endocrine neoplasia, it ought to not be used in people with a previous or household history of such problems [59-- 61] The most popular strategies concern unimolecular combination of GIP and/or glucagon receptor (GcgR) agonism with extremely potent, corresponding GLP1R agonism. GIPR agonists, as soon as chemically incorporated with GLP1R agonism, have demonstrated metabolic benefits and decreased body weight in computer mice when compared with pharmacokinetically matched GLP1R agonists122,189. There are multiple reasons GIP agonism could give supplementary metabolic advantages to GLP1 treatment, apart from lowering body weight and food intake via GLP1R-independent mechanisms184,185. GIP obstructs the emetic impacts of GLP1R agonism in musk shrews190 and near-normalization of blood sugar has been reported to restore the insulinotropic impact of GIP in patients with T2D191. Moreover, GIP agonism improves adipocyte storage ability to secure from adipocyte lipid overflow and ectopic lipid deposition192. Nonetheless, as discussed in the preceding subsection, the use of GIPR agonists for the treatment of weight problems and Visit this website T2D is controversial. 
Social Links